Boxer’s knuckle, medically termed as sagittal band rupture, is a condition predominantly affecting athletes, particularly boxers, but can also occur in individuals engaged in activities involving repetitive stress on the hand and fingers. This condition involves a tear or disruption of the sagittal band (described below) at the base of the finger, typically the middle finger, resulting in pain, instability, and reduced function of the affected digit.
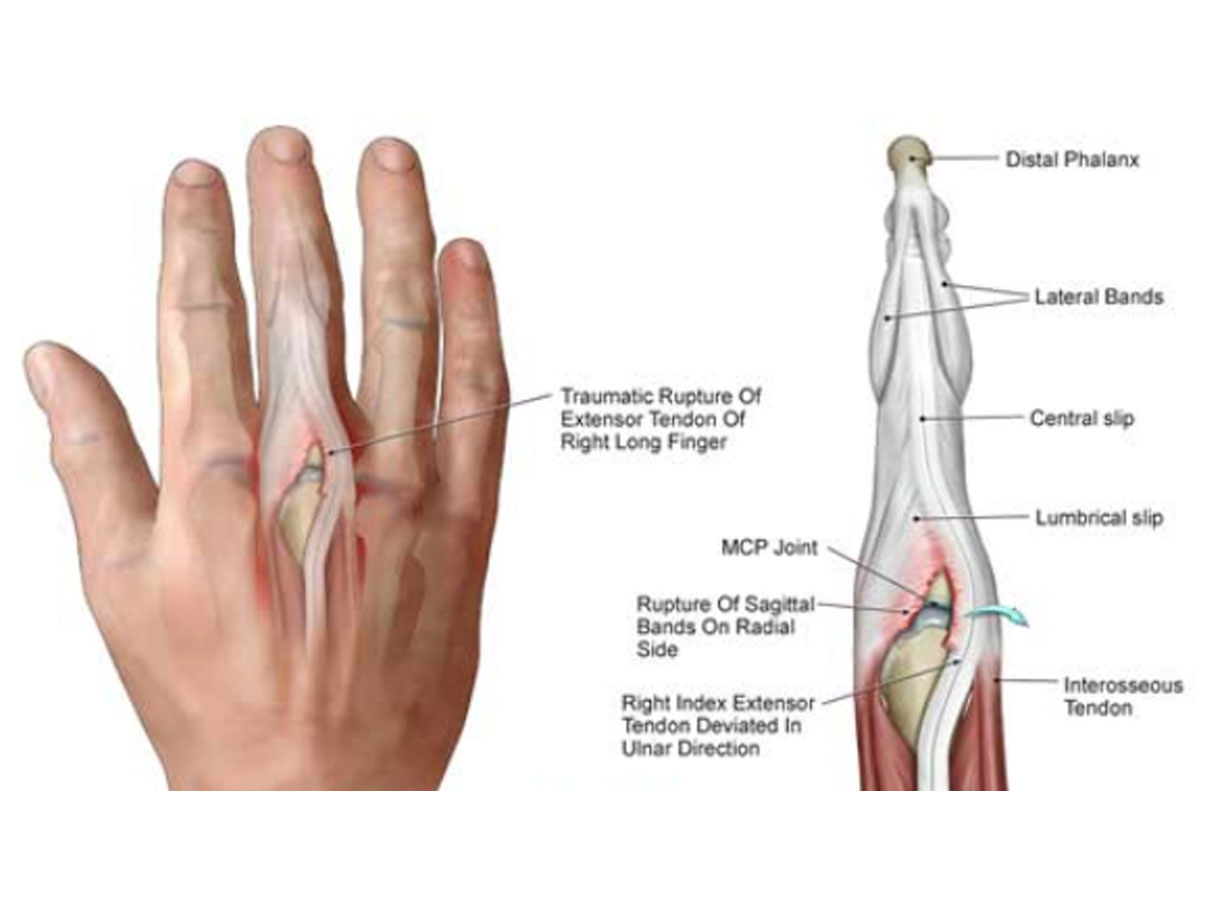
Anatomy
- Repetitive Trauma: Frequent and forceful impact on the hand and fingers, as seen in boxing, martial arts, or other contact sports.
- Improper Technique: Incorrect punching techniques, inadequate hand protection, or training errors can increase the risk of developing this condition.
- Occupational Factors: Certain occupations involving repetitive hand movements or trauma may predispose individuals to boxer’s knuckle.
Signs and Symptoms you may notice and experience.
- Subluxation (movement out of its regular position) of the extensor digitorum tendon during bending of the finger.
- Pain: Localized pain at the MPJ.
- Swelling and Instability: Swelling around the affected joint with potential joint instability, leading to difficulty in performing daily activities.
- Reduced Range of Motion: Limited ability to extend the affected finger fully.
- Visible Deformity: In severe cases, a visible deformity or palpable gap at the base of the affected finger may be present. There may also be bruising.
Diagnosis and Assessment
In order to get an accurate diagnosis, your attending physio will conduct a thorough clinical evaluation including history and physical examination. Imaging studies like X-rays or ultrasounds are important to rule out a fracture in the light of trauma, and to confirm the suspected diagnosis. Your physiotherapist will attend to there referrals.
Surgical management
In cases where there is significant tearing of the sagittal band, surgical repair may be necessary and your physiotherapist will refer you to a hand specialist.
Physiotherapy Management
Initial management involves rest, ice, compression, and elevation (RICE) to alleviate pain and swelling. Immobilization with splinting or taping may be recommended to stabilize the joint. All of the aforementioned is promote the healing of your tissue. Physiotherapy plays a crucial role in the rehabilitation process, focusing on:
- Relative rest: Strengthening of the surrounding muscle groups without causing pain so as to allow the injured tissue to heal.
- Technique: It is important that the correct punching technique be encouraged so as to prevent re-injury.
- Manual Therapy: Soft tissue mobilization, joint mobilization, and therapeutic exercises to restore joint function and flexibility.
- Functional Rehabilitation: Functional exercises tailored to the patient’s specific needs and activities to restore normal hand function.
If this blog sets off a lightbulb, do not hesitate to get your hand evaluated by one of our highly experienced physiotherapists.
References
Gladden, J.R. (1957) ‘Boxer’s Knuckle’, The American Journal of Surgery, 93(3), pp. 388–397. doi:10.1016/0002-9610(57)90828-0.
Hame, S.L. and Melone, C.P. (2000a) ‘Boxer’s Knuckle’, Hand Clinics, 16(3), pp. 375–380. doi:10.1016/s0749-0712(21)00579-5.
Hame, S.L. and Melone, C.P. (2000b) ‘Boxer’s knuckle in the professional athlete’, The American Journal of Sports Medicine, 28(6), pp. 879–882. doi:10.1177/03635465000280061701.
Mok, K. (2006) ‘Boxer’s knuckle of Non-Boxer patients’, Hong Kong Journal of Emergency Medicine, 13(3), pp. 161–167. doi:10.1177/102490790601300306.
Watté, N., Walschot, L. and Vanhoenacker, F. (2021) ‘Boxer’s Knuckle’, Journal of the Belgian Society of Radiology, 105(1). doi:10.5334/jbsr.2620.