Description
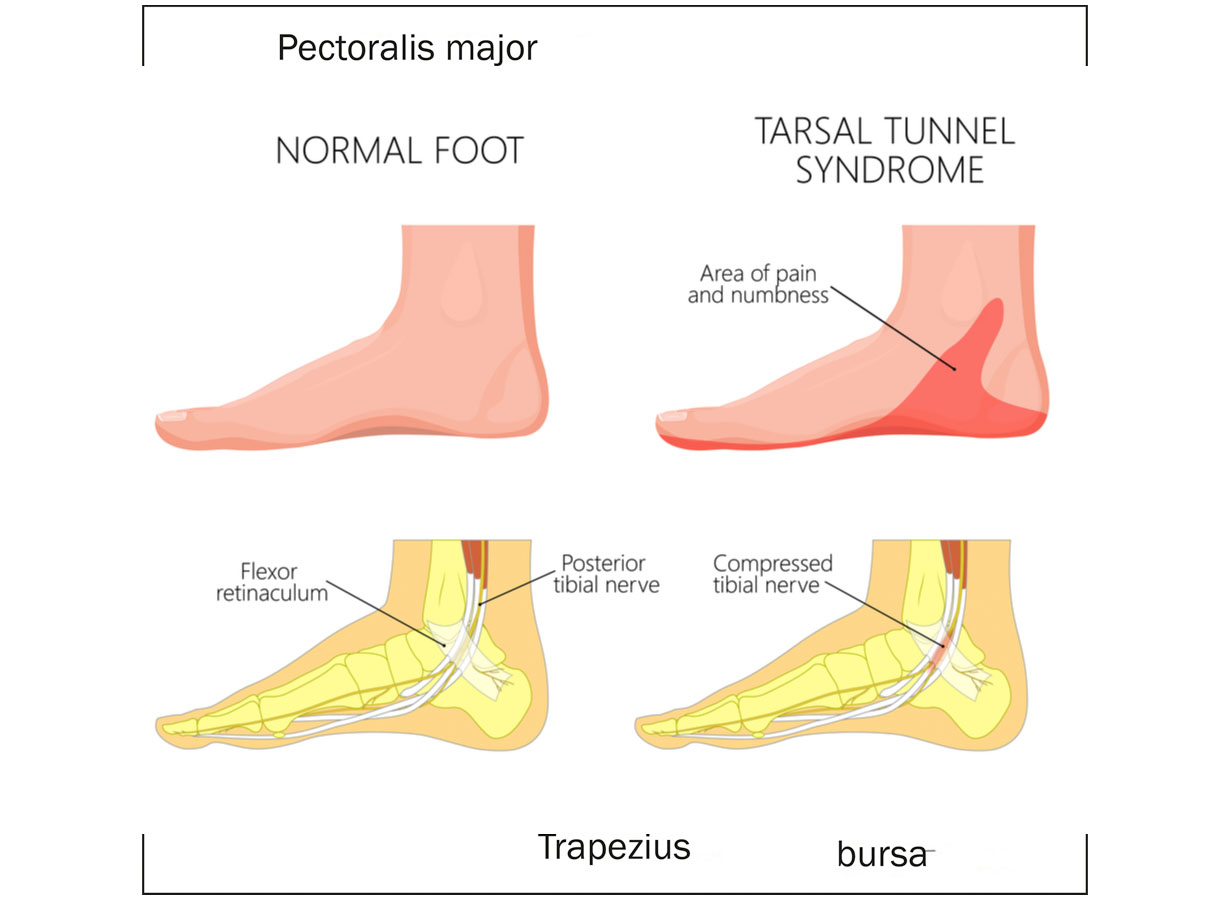
Tarsal tunnel syndrome (TTS) is a condition in which the tibial nerve or 1 of its terminal branches is compressed within the tarsal tunnel of the medial malleolus (inner ankle bone).
Anatomy
The tarsal tunnel is formed by a bony floor and a connective tissue roof. The floor is concave and formed by the medial/inner tibia, talus/ankle bone and calcaneus/heel bone. The roof is formed by the flexor retinaculum which is a fibrous tissue that runs from the medial malleolus to the calcaneus.
What are the contents of the tarsal tunnel
- Tibialis posterior tendon
- Flexor digitorum longus tendon
- Flexor hallucis longus tendon
- Posterior tibial artery
- Tibial nerve
What are the associated Risk factors?
- Extra and accessory muscles around the ankle – flexor digitorum accessorius longus muscle, tibiocalcaneus internus muscle or accessory soleus.
- Chronic instability of the ankle.
- Surgical procedures to correct angulation of the hind foot.
What are the signs and symptoms?
- Paraesthesia in the heel, medial ankle and under surface of the foot.
- Aggravation of the above symptoms with activity and ease with rest.
- Paraesthesia whilst sleeping with the foot in certain positions.
- Wasting/atrophy of muscles on the underside of the foot.
- Weakness of the above muscles.
Assessment
Diagnosis of TTS is mainly based on clinical examination. This includes a series of special tests. Due to strength and range deficits which tarsal-tunnel syndrome could cause, it is also essential to assess range of motion at the ankle and strength of the surrounding muscles. When there is a high index of suspicion for this condition, your attending physiotherapist should send you for nerve conduction tests.
What does treatment consist of?
- Activity modification and relative rest.
- Optimal loading.
- Ice, compression and elevation.
- Orthotics if applicable.
- Appropriate footwear selection.
- Active range of motion exercises of the foot and ankle
- Strengthening of foot intrinsic muscles
- Strengthening of larger muscle groups – calf and tibialis anterior.
Surgical intervention
If conservative management does not provide optimal symptom relief, surgical intervention must be considered. Operative management consists of decompression of the nerve within the tarsal tunnel. The surgeon releases the nerve of any structure which is causing compression. Post operative management will look to address any deficits as a result of the surgery.
References
Fortier, L., Leethy, K., Smith, M., McCarron, M., Lee, C., Sherman, W., . . . Kaye, A. (2022). An Update on Posterior Tarsal Tunnel Syndrome. Othopaedic Reviews, 14(3), 1-8.
Gallas, J., & Gearhart, M. (2015). Conservative Management of Tarsal Tunnel Syndrome in a Competitive Distance Runner. Orthopaedic Practice, 27(2).
Gretter, T., & Wilde, A. (1970). Pathogenesis, diagnosis, and treatment of the tarsal-tunnel syndrome. Cleaveland clinic Foundation, 37, 23-29.
Kushner, S., & Reid, D. (n.d.). Medial Tarsal Tunnel Syndrome: A Review. The Journal of Orthopaedic and Sports Physical Therapy, 6(1), 39-45.
Romani, W., Perrin, D., & Whiteley, T. (1997). Tarsal Tunnel Syndrome: Case Study of a Male Collegiate Athlete. Journal of Sports Rehabilitation, 6, 364-370.